|
LITUANUS
LITHUANIAN QUARTERLY JOURNAL OF ARTS AND SCIENCES
Volume 28, No. 4 - Winter 1982
Editor of this issue: Jonas Zdanys, Yale University
ISSN 0024-5089
Copyright © 1982 LITUANUS Foundation, Inc.
|
|
HEART DISEASE IN THE BALTIC STATES: A PERSPECTIVE
JOSEPH A. STANKAITIS, M.D.*
Beginning around the post-World War II era, the incidence and mortality associated with coronary artery disease demonstrated a rapid and progressive rise in the United States and the Western World. This epidemic reached its highest level in the late 1960's with a reversal of this trend since that time where the age-adjusted overall mortality due to coronary artery disease declined by over 20 per cent in the United States between 1968 and 1976.1 This trend is shown in Figure
1.2 There is strong suggestion that
improvements in risk factors such as diet, decreased cigarette smoking, control of hypertension, and a greater emphasis on physical activity have played a significant role in curbing this disease of epidemic proportion.
Revisions of the International Classification of Diseases
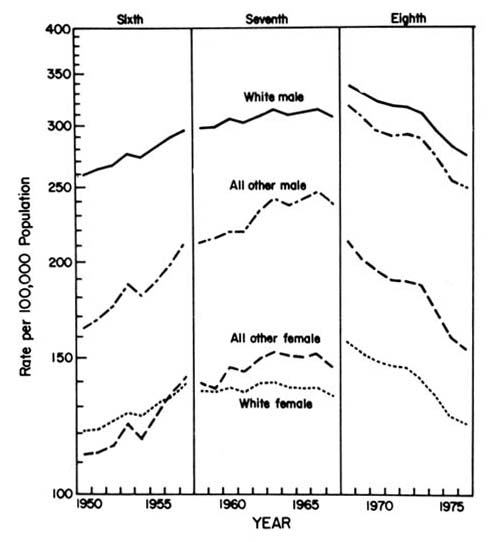
Figure 1. Age-adjusted death rates for ischemic heart disease by color and sex: United States, 1950-1976.
Unfortunately, the Soviet Union currently finds itself in a situation where its crude death rates have sustained a 42 per cent increase from 1964 to 1978.3 Although the Soviet Union
does not report its statistics completely to the World Health Organization and its data is relatively scanty internationally, it is felt that once vital statistics have been examined (See Figure 2), coronary artery disease accounts as the primary cause for the rising death rates within the Soviet Union.
CRUDE DEATH RATES IN THE SOVIET UNION FROM 1960 to 19774
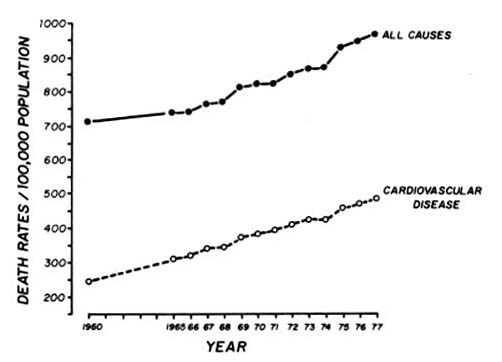
Figure 2
This current epidemic is taking a heavy toll within the Baltic States. Vikhert, et. al, found that the large citites within the Russian Soviet Socialist Republic and the Baltic states of Lithuania, Latvia and Estonia have rates of coronary artery disease far and above those found in Siberia, Central Asia and Caucasus.5 An autopsy study comparing the five
towns of Tallin (Estonia), Yalta (Ukraine), Ryazan (rural Russia), Prague, and Malmo (Sweden) revealed a higher incidence of atherosclerotic coronary artery disease among both men and women in Tallin than in the other Soviet towns.6
Given these findings, the people of the Baltic states, let alone those of the Russian Soviet Federated Socialist Republic, are confronted with an extremely serious health problem that should warrant immediate attention. Unfortunately, at least for the present time, very little action has been demonstrated or planned by the Soviet Government to help rectify this situation.7
Given whatever data is available and our understanding of this disease process, one can examine some of the possible reasons for this epidemic and speculate on its impact upon the Baits.
It is generally felt that among all the republics within the USSR, Lithuania, Latvia and Estonia are probably the most "westernized." People from outside the Baltic region within the USSR tend to visit this area since it affords them a glimpse of the Western World that they customarily are unable to experience. As noted by western journalists, there exists a heavy Soviet economic investment and a relatively high level of productivity in this region which gives the Baits the highest living standards in the USSR.8 Thus, one could see that although under "eastern" domination there is a westernized life style of sorts present in the Baltic states. Consequently, this living and "the good life" likewise carries some of the inherent risk factors of coronary artery disease experienced by the West during the period of increase of disease in the post World War II era.
With increased economic industrialization, the Baits experienced a major shift in population. While traditionally
a rural peoples, since World War II the Baltic population has become heavily urbanized. This fact in and of itself increases the incidence of heart disease as shown by Vikhert and Sedov who demonstrated that the prevalence and extent of coronary artery disease was significantly lower in rural than urban subjects in the USSR.9
Although there was a population shift from rural to urban, diet within the Baltic states has failed to change. This diet, based upon staples available on the farm, remains traditionally the same with an inordinately high intake of saturated fats and dairy products. Although dietary changes with greater use of polyunsaturated fats and weight control have been attributed as a significant cause for the impressive decline in heart disease in the United States, no such similar change appears on the horizon for the Baltic peoples. There is little discouragement of obesity and one wonders if such a campaign would ever be accepted in the present milieu of highly publicized food shortages in Eastern Europe. The combination of decreased physical activity (via urbanization) with maintenance of an atherogenic diet could very well prove to be quite significant if the recent studies examining the effect of exercise and diet in primates is applicable to humans.10
Cigarette smoking has been well recognized as a risk factor for the development of coronary artery disease. Even though Lenin himself was opposed to smoking, the consumption of cigarettes within the USSR is fairly universal. Some estimates have indicated a prevalence, for example, of as high as 70 per cent of the male population of Moscow engaged in cigarette smoking.11 Needless to say, there has been little discouragement of this practice (even Leonid
Brezhnev smokes publicly) with no educational or generalized preventative activity planned for the future.
Arterial hypertension remains a classical risk factor for heart disease. Its prevalence in middle-aged groups throughout the Soviet Union has been estimated at about the 30 per cent level with only 5 to 13 per cent of those within that group receiving adequate therapy.12 This consequently leaves untreated a sizable portion of the population with a highly treatable risk factor. The American Heart Association has focused its efforts on the detection and treatment of high blood pressure with results that strongly suggest a significant contribution to a decrease in stroke and heart disease in the U.S. population. Unfortunately, such a widespread program does not currently exist in the Baltic Region, let alone the rest of the USSR.
Zyzanski, et. al. have shown angiographically that intense and sustained disturbing emotions such as anxiety and depression are associated with the artherosclerotic process and not merely related to the intensity of complaints in reference to these symptoms.13 It might very well be postulated that there indeed must exist a significant amount of anxiety and depression within the USSR including the Baltic states as manifested by the widespread problem of alcohol abuse.14 The Russian psychiatrist, Boris Segal, has noted that "the growth of drinking during the Soviet period (of Russian History) is also connected with the economic deprivation of the majority of the Soviet population, the suppression of personality, private initiative, and spiritual freedom. These produce a growth of alienation,
dissatisfaction, feelings of insecurity, anger and escapist tendencies."15 Alcoholism continues to be a rampant problem within the Baltic states. Thus one could be able to make a case for the existence of a significant level of intense and disturbing emotions within the Baltic states which may further translate into a significant contributory cause of coronary artery disease.
We can thus see that the Baltic states as a people are faced with a serious health problem of multifactorial origins. One would believe that the Marxist-Leninist society under which they live would be able to easily implement a systematic program aimed at correcting the numerous risk factors for heart disease that presently plague these peoples. Educational programs for the detection and treatment of hypertension, for proper diet and fitness, and for prevention of cigarette smoking have been instituted in the U.S. with proven effectiveness.
Furthermore, with the advent of newer cardiac drugs such as Propranolol and Timolol, there is a strong suggestion, although not yet proven, that these agents will make a greater impact on mortality due to coronary artery disease at least in the United States. Use of such medications should likewise prove useful to the Baltic and Soviet populations.
One could hope that those presently governing the Baltic states would take a long and hard look at this current health crisis and realize that to better the welfare ot these people and all the peoples of the USSR it will necessitate a commitment not only at the scientific level but also at the political level. Our hope is that it will not be a difficult choice to make.
* Dr. Stankaitis is Assistant Clinical Professor of Medicine, University of Rochester School of Medicine, and Co-Director of the Division of Internal Medicine of the Department of Medicine at the Genesee Hospital in Rochester, New York.
1 Stern MP. The recent decline in ischemic heart disease. Annals of Internal Medicine 1979; 91: 630.
2 Division of Vital Statistics, National Center for Health Statistics. Chartbook for the Conference on the Decline in Coronary Heart Disease Mortality, Hyattsville, Maryland, U.S. Dept. of Health, Education and Welfare, August 1978.
3 Cooper R. Rising death rates in the Soviet Union.The impact of coronary heart disease. New England Journal of Medicine 1981; 304: 1259.
4 Dutton J Jr. Changes in Soviet mortality patterns, 1959-1977. Population and Development Review. 1979; 5: 267-291.
5 Vikhert AM, Sedov KR, Sokolova Rl. Comparative characteristics of aortic and coronary atherosclerosis found in populations of
Irkutsk, Kharkov, Baltic Republics and Middle Asia, Cor Vasa 1970; 12: 12-26.
6 Vanecek R. Atherosclerosis of the coronary arteries in five towns. Bulletin World Health Organization 1976; 53: 509.
7 Field MC. Powell DE. Alcohol abuse in the Soviet Union. The Hastings Center Report 1981; 11: 40.
8 Knight R. US News and World Report 1978; 85: 43-4.
9 Vikhert AM, Sedov KR. Kardiologija (Moscow) 1969; 5: 18.
10 Kramsch DM, Aspen AJ, Abramowitz BM, Kreimendahl T, Hood WB Jr. Reduction of coronary artherosclerosis by moderate conditioning exercise in monkeys on an atherogenic diet. New England Journal of Medicine 1981; 305: 1483.
11 Cutting Tobacco's Toll. Washington, D.C. Worldwatch Institute, 1978, 18.
12 Mazur NA. Report from Union of Soviet Socialist Republics. Cardiovascular Epidemiology Newsletter, 1979; 16: 25-35. (Dallas: Council on
Epidemiology, American Heart Association).
13 Zyzanski SJ, Jenkins CD, Ryan TJ, Flessas A, Everist EM. Psychological correlates of coronary angiographic findings. Archives of Internal Medicine 1976, 136: 1234-7.
14 Segal BM. Drinking patterns and alcoholism in Soviet and American societies: A multidisciplinary comparison. Psychiatry and Psychology in the USSR. Corson SA, editor, Plenum Press, New York. 1976: 181.
15 IBID, p. 181.