|
LITUANUS
LITHUANIAN QUARTERLY JOURNAL OF ARTS AND SCIENCES
Volume 49, No.1 - Spring 2003
Editor of this
issue: Violeta Kelertas
ISSN 0024-5089
Copyright © 2003 LITUANUS Foundation,
Inc. |
|
SELLING MADNESS: PSYCHOPHARMACEUTICAL COMPANIES IN
LITHUANIA, 1990-2000
VINCENT GIEDRAITIS
University of California, Riverside
Let us ever hold fast to what it is to be a human
being.
Soren Kierkegaard
Only science, exact science about the human self, and
the most sincere approach to it by the aid of the omnipotent scientific
method, will deliver man from his present gloom, and will purge him from his
contemporary shame in the sphere of inter-human relations.
Ivan Petrovich Pavlov
INTRODUCTION
The breakup of the Soviet Union has created enormous
tensions, both economic and cultural, for its former member states. Once under
the watchful and guiding eye of the Soviet Union, the former republics suddenly
had to determine how to react to an increasingly integrated global economy.
Lithuania, since its reestablishment of independence in 1991, has been torn
between the legacy of Communist influence from the East, and cultural and
economic pressures from the West. As I will show, Western influences have led to
major changes in Lithuanian mental health. Lithuania has experienced a sharp
increase in certain types of mental illness between 1997 and 1998, as indicated
in Table 1.*
TABLE 1.
Rates per
100,000 of Specific Mental Disorders and % Change
| Disorder |
ICD-10
Code |
1997 |
1998 |
% Change |
Organic, including symptomatic
mental disorders. |
F00-F09 |
23.8 |
45.5 |
+91.2% |
| Schizophrenia. |
F20-F29 |
23.8 |
27.5 |
+15.6% |
| Mood (Affective) disorders. |
F30-F39 |
25.1 |
101.6 |
+305.0% |
| Neurotic and Stress-related disorders. |
F40-F49 |
16.1 |
24.3 |
+50.9% |
Behavioural syndromes associated
with physiological disturbances
and physical factors. |
F50-F59 |
0.6 |
1.8 |
+200.0% |
Disorders of adult personality
and behaviour. |
F60-F69 |
8.2 |
9.3 |
+13.4% |
Source: Lithuanian Ministry of
Health.
*Having gathered this data
during the Summer of 2000, I was unable to expand upon this two-year
period, since I am unable to find this information in the United
States. According to information provided by the Vilnius Psychiatric
Clinic, http://www.sam.lt/statistics/tablel4.htm, incidence of
affective mood disorder in the mental health system increased from
25.1 to 101.6 per 100,000 people between 1997 and 1998.
The question driving this research is why rates of mental
illness in Lithuania have increased so rapidly in the 1990s in light of the
rising influence of Western pharmaceutical companies. These firms expanded their
marketing strategies in Lithuania, since it became an untapped market after the
fall of the Soviet Union. Using both formal and informal means, the
pharmaceutical industry influences the diagnosis of various types of mental
illness treated by medications sold by these same pharmaceutical companies.
While other scholars have stressed the role of the
interaction process between individuals, this research contributes to the debate
of the social construction of mental illness by emphasizing the macroeconomic
sources of the diagnosis of mental illness.
The Social Construction of Mental Illness
This section provides a brief overview of three general
perspectives on mental illness, and indicates ways in which this paper fits
within and contributes to these established paradigms. My argument for a
relationship between increasing rates of mental illness and the expanding market
of foreign pharmaceutical companies draws upon labeling theory and the
antipsychiatric school of thought.
Labeling theory is based on one
fundamental idea: those who are labeled deviant and treated as such will become
deviant (Scheff 1974, Lemert 1951, Lemert 1972, Becker 1973). By extension,
those who are treated as mentally ill will come to act mentally ill, thereby
beginning a self-perpetuating cycle. For labeling theorists, mental illness does
not exist in the sense proposed by those who embrace a medical (or "biological")
model, which sees mental illness as a physiological phenomenon that should be
treated like any other disease. Mental illness is fundamentally a social
phenomenon for labeling theorists and for those who refer to the
"medi-calization" of mental illness. Both see mental "health" as being an
arbitrary condition (Conrad 1975, Szasz 1963, Scull 1975, Laing 1967, Goffman
1959). Behavior becomes socially constructed, as proposed in the "radical"
perspective of the antipsychiatrists (so-called due to their opposition to the
medical model), using the legitimacy of the medical institution as an agent of
social control (Conrad 1980, Szasz 1963). Psychiatrists such as Laing
(1967,1969) and Szasz (1974), who argue that mental illness does not exist at
all, represent the extreme fringe of the antipsychiatric model. While Laing sees
schizophrenia as a "sane reaction to an insane world," Szasz sees mental illness
as a medical "myth," because there are no signs of physical lesions. What is
missing from this perspective is a macro-level analysis that emphasizes economic
factors.
The above-mentioned researchers focus on a micro context.
My research contributes to their paradigms by proposing that mental illness is
intimately tied to large economic processes. I examine how the social
construction of mental health at the micro level is shaped by macroeconomic
conditions, specifically, the rise of capitalist drug companies in Lithuania in
the context of an increasingly integrated capitalist world economy.
THEORY
I hypothesize that Western pharmaceutical companies seeking
new markets for their medications are in effect creating a demand for their
products, which, in turn, leads to increasing rates of diagnosed mental illness.
Theoretically, my project contributes to the field of social psychiatry by
linking psychiatric diagnoses to economic changes. Also, the issue of what
underlies mental health sociologically has practical implications, both in
Lithuania and the United States, for at least two reasons. First, how mental
health is defined sets the stage for research agendas and policy issues. For
example, if mental illness is deemed a mainly physiological phenomenon, as was
the case in the Soviet Union, then biological treatment makes sense. Yet if
mental illness is seen as having both social and biological causes, then a blend
of treatments, both social and physiological may be useful. Second, how mental
illness is defined also impacts the way mental patients view themselves, which,
in turn, influences their coping strategies (Townsend 1975, Karp 1996). Third,
how psychiatrists view and treat mental patients is related to determining the
cause of their afflictions.
This study not only contributes to sociological literature
on Lithuania and Eastern Europe, but is relevant to psychiatric processes in the
United States and other capitalist countries as well. As the markets that
psychiatry comes to dominate expand, consumers and society as a whole must
become increasingly aware of the possible dangers in this domination.
Sociologists must be aware of and investigate the social nature of mental
illness and the relationship between the legitimacy of the medical model and
economic and cultural factors supporting that legitimacy.
Figure 1 models the hypothesized relationship between
capitalist development and increasing rates of mental illness. Drawing on
world-systemic explanations of a global capitalist economy (Chase-Dunn 1982;
Chase-Dunn and Boswell 1998), I argue that Western capital influences the
operation of pharmaceutical companies. These firms, which must operate
profitably, do so by marketing their products aggressively. Western
pharmaceutical companies entice Lithuanian psychiatrists to prescribe more
pharmaceuticals, which increases both the profits of the pharmaceutical
companies and the official rate of mental illness.
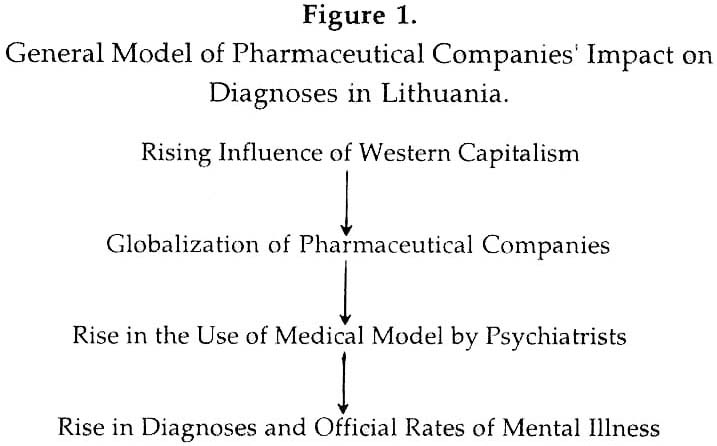
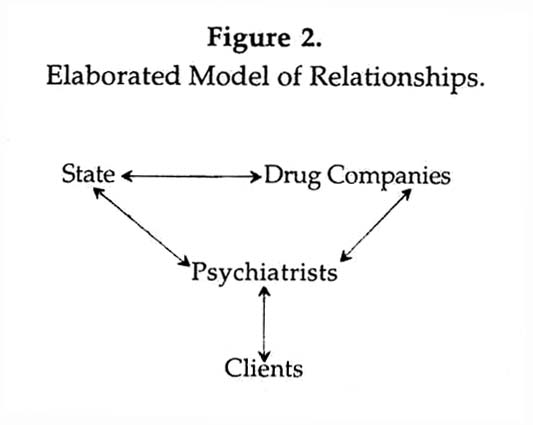
Figure 2 diagrams a more elaborate model that illustrates the relationship
between the discussed variables. It indicates that there is a complex
interrelationship between several important factors. The state is interested in
saving money in its health care system, and, therefore, minimizes the use of
expensive treatments, such as traditional "talking" psychotherapy. Drug
companies seek to maximize their profits. Both the state and the drug companies
influence the psychiatrists who deal with clients/patients. Though psychiatrists
determine the diagnosis, patients may come to them already seeking medication.
Lithuania is a fruitful choice for studying the effects of capitalist
development on rates of mental illness, because it has experienced a sharp rise
in the influence of capitalism during the past ten years. One would expect the
reforms in psychiatry enacted in Lithuania to increasingly resemble those
observed in a capitalist system. This study is a timely one. The breakdown of
the Soviet Union in 1990 has led to a major transformation in formerly socialist
societies. The breakup of the Soviet Union has created new markets for foreign
investors eager to sell products and services to people used to living under
communism.
Lithuania's Post-Socialist Economy and Capitalist Influences on Mental
Illness
Following the collapse of the Soviet Union, Lithuania's economy converted from
the socialist command economy to a capitalist-oriented market economy. There is
much discussion within social and economic theory describing the Eastern
European economic transition. Szelenyi (1998) built upon the work of Polanyi
(1951) in seeing distinct stages in the transition from state socialism to the
development of a market economy with capitalist institutions. The key factor,
Szelenyi argues, is the role of business in consciously creating and expanding
capitalist markets in Eastern Europe. My research draws from Szelenyi's argument
by indicating the role of drug companies with the help of psychiatrists in
consciously expanding their markets.
Health is related to the economic transition. Brainerd (1999) indicates that
there is a relationship between the market reform of Eastern and Central
European nations and mortality rates in those countries. Although the money that
the Baltic Republics can spend on health and social services is mediated by many
social and economic factors, the amount spent is related to the government's
annual revenue.
My research suggests that, when faced with difficult economic choices, the
Lithuanian government seeks to address the health care needs of the population
(e.g., a very high suicide rate) with the most cost-effective means possible
(medication, as opposed to psychotherapy).
In this section, I will review different perspectives on the relationship
between psychiatry and capitalism. Unlike a capitalist economic system, the
Soviet-style command economy fostered no profit motivation for markets to
expand.
Under capitalism, psychiatry operates on a for-profit basis. One implication of
this is unequal access to quality treatment. For example, Garfield (1994)
indicates that the upper classes receive far better psychiatric care than the
lower classes in the United States. He suggests that the treatment given to the
upper classes is based on insight and inner understanding, while that given to
lower socioeconomic groups is based on chemical pacification and containment.
This type of care is by far much more expensive than simply medicating a
patient, which appears to be the more common practice in Lithuania.
Bryan Turner (1995) points to the increasing globalization of Western medical
knowledge. He discusses medical knowledge in theory, but does not address the
complex interplay between professional psychiatric organizations and capitalism.
According to U'ren (1997) both capitalism and psychiatry are interested in
expanding their markets. U'ren draws upon Marxist conceptions of economics in
capitalism, using Marx and Engels' (1848/1948) notions of capitalist
competition, where capitalists create a "market" for the psychopharmaceutical
industry. Using the Marxist M1-C-M2 formula, an initial
investment (M1) leads to a commodification (C), which is then sold
for profit (M2). This profit is then reinvested for more profit as
the cycle continues. In short, in order to create a profit, goods must be
marketed.
Foucault (1965) also saw socioeconomic factors as influencing the conception of,
and creation of, mental illness. He argues that as the industrial revolution
brought new era thought about the mentally ill, the rhetoric used to discuss the
mentally ill changed: the "village idiot" began to be identified as a patient.
Foucault finds no surprise that the industrial revolution brought with it the
first asylums for the mentally handicapped, as the need for increasingly
reliable labor became important. Although Foucault focuses on the relationship
between discourse and economic factors, he sees the economy as a unit, rather
than a set of competing interests that seek profit through labeling some as
mentally ill. While U'ren sees psychiatry as operating along with the capitalist
economic system, Foucault sees demeaning language as being an indirect cause of
the changing economic systems. In contrast to Foucault, who emphasizes the
capitalists' interest in maintaining a steady supply of reliable labor, I focus
on the need to expand drug markets, which encourages the labeling of people as
mentally ill.
Though my research draws upon aspects of all the mentioned theorists, it most
closely resembles the claims made by U'ren. However, while U'ren focuses on
diagnostic criteria, I see psychiatrists as the middlemen between larger
capitalist economic forces and the official rates of psychiatric disorder they
create. What is missing from U'ren's discussion is the way that psychiatry
expands its markets and the role drug companies play in this expansion.
My research further indicates that mental illness is created through economic
processes. Various researchers see the major diagnostic tool used by American
psychiatrists, the Diagnostic and Statistical Manual, as creating mental illness
through its use of categories, labeling the afflicted, and treating behavior as
signs of mental illness (Sands, 1983; Mi-rowsky, 1989).
Methods
Three primary sources of data will be utilized to support my argument:
interviews with various individuals associated with the mental health care
system, government statistics, and archival data. Most of the archival materials
consist of Lithuanian news articles from the Mazvydas Library and the Vilnius
Medical Library.
This extended case study focuses on developments in Lithuanian psychiatry in the
period from 1990 to 2000. 1990 is the year Lithuania first began to take clear
steps towards independence on the world stage. Through interviews, I was able to
see the world thorough the eyes of Lithuanian psychiatrists. Those interviewed
were found by using the "snowball" approach. From a personal contact in Los
Angeles, who had finished medical school in Vilnius, I was able to interview her
former professor, who is now the current dean of the University of Vilnius
medical school. This contact, in turn, led me to other psychiatrists in
Lithuania, and so on.
Some of those interviewed, such as the dean of the Vilnius medical school,
offered perspectives from a position of power within the health care system.
Another psychiatrist interviewed was the director of a state-run clinic, while
others were former presidents of the Lithuanian Psychiatric Association. Lastly,
some psychiatrists were physicians employed by various state-operated clinics,
which constitute the bulk of psychiatric clinics in Lithuania.
Interviews were conducted in an unstructured format, and all conversations took
place in the Lithuanian language. Five individuals were interviewed during the
summer of 2000: four psychiatrists and a Baltic representative for the
pharmaceutical company Eli Lilly. Open-ended questions were asked; interviews
typically lasted from one hour to an hour and a half. Three general topics were
discussed in interviews: the respondents' accounts of the economic transition to
capitalism, the role of medication versus psychotherapy, and Western
pharmaceutical companies' influence on psychiatry in Lithuania.
The government statistics used to support my conclusions were obtained from the
Lithuanian Ministry of Statistics and, in the case of diagnoses of specific
types of mental illnesses, from the Vilnius Psychiatric Clinic. Archival data
were used for general background information on changes in government policy on
mental health and public perceptions of mental illness.
FINDINGS
This section is organized around several dominant themes appearing in the data.
First, recent trends in Lithuanian mental health care will be discussed, in
addition to current rates of mental illness. As will be indicated, the
government's need to save money, the prior dominance of the medical model under
Soviet rule, and the perception of suicide as a public health problem have all
had an impact on rates of mental illness. Next, an argument is presented about
the means by which pharmaceutical companies influence rates of diagnosis of
mental illness.
Recent Trends in Lithuania's Mental Health
Since re-independence, Lithuania's Ministry of Health began to gather its own
health statistics. Table 1 indicates the total number of reported cases of
mental disorders in the records of the Ministry of Health for the years 1997 and
1998 for all types of mental illness. As is evident, the rates of increase are
high—up to 305% for affective mood disorders— from 1997 to 1998. How can such
rapid increase be explained?
The "Courting" of Lithuanian Psychiatrists
Drug companies in Lithuania use aggressive marketing techniques. The conference
Depresija 1995 (Depression 1995) was sponsored exclusively by Eli Lilly, and the
2000 National Suicide Conference was cosponsored by Eli Lilly. These conferences
served several purposes. According to an Eli Lilly representative, "Doctors came
and learned about depression and its treatment." Psychiatrists indicated that
drug companies actively encourage doctors to attend conferences through informal
enticements. The dean of the medical school told me:
They sent doctors to conferences. The firms organized
these conferences. Sometimes they were close to ballets. The doctors that
went were made to feel good, so that they would want to go. There is a turn
to bio-psychology, away from psychotherapy.
When asked about the Depresija 95 conference, a psychiatrist came to a similar
conclusion:
Eli Lilly organized it. It was in Kaunas [The second
largest city in Lithuania]. It was the debut of Prozac [in Lithuania]. The
Prague theater was there. The pharmaceutical industry invited doctors. It
was like a big party, a big deal.
Though such perks are common to medical conferences in the Unites States, one
must remember the cultural and temporal context in which this "courting" is
taking place. During the Soviet era, Lithuanian medical doctors were (and
continue to be) paid very little relative to their Western counterparts.
According to government statistics, in 1997, the average worker in Lithuania
earned 785 litas (approximately 196 USD) per month, whereas those engaged in
human health activities earned only 640 litas (approximately 160 USD) per month.
In 1997, doctors and other medical personnel earned, on average, the same amount
per month as those engaged in sewage and refuse disposal (Statistical Yearbook
of Lithuania, 1999).
Psychiatrists in Lithuania enjoy going to corporate-sponsored conferences very
much. For them it is a taste, perhaps the only taste, of the "good life." As
Western culture becomes increasingly visible in Lithuania, doctors would be
expected to desire the cultural and material rewards associated with the medical
profession in the West. The amount drug companies spend on conferences is only a
fraction of the amount earned from the potential sales of pharmaceuticals.
When asked if drug companies can find out if particular doctors use certain
products, a psychiatrist responded, "Yes. It's all in the books." Thus,
informally, drug companies are able to "reward" doctors that prescribe their
drugs through conference invitations. It seems that drug companies are
"enticing" psychiatrists to prescribe medications, which is, in turn, reflected
in the increasing diagnoses of mental illness.
Lithuania's High Suicide Rate as a Public Health Problem
A second explanation of why drug companies have been able to market their
products so easily in Lithuania revolves around the high incidence of suicide in
the country. Before the Soviet occupation, Lithuania's suicide rate was among
the lowest in the world. However, as Table 2 shows, the rate steadily increased
during the Soviet era and is now among the world's highest. Table 3 shows
Lithuania's suicide rate compared to several other nations.
TABLE 2.
Total Number and Rate of Suicides in Lithuania.
| Year |
Total |
Rate per
100,000 |
| 1990 |
969 |
26.0 |
| 1991 |
1142 |
30.5 |
| 1992 |
1294 |
34.6 |
| 1993 |
1572 |
42.1 |
| 1994 |
1703 |
45.8 |
| 1995 |
1694 |
45.6 |
| 1996 |
1723 |
46.4 |
| 1997 |
1632 |
44.0 |
| 1998 |
1554 |
42.0 |
Source: Lithuanian Ministry of Health.
Various explanations have been offered for this high rate. One supposes that the
rapid pace of social and economic change in Lithuania, following its
independence has caused an increase in anomie. Another reasons that it is
related to Lithuania's high rate of per capita alcohol consumption, which
historically has been roughly proportional to rates of suicide. As shown,
compared to other nations, even those close by, such as Estonia, Lithuania's
suicide rate is very high.
TABLE 3.
Suicide rate per 100,000 for Selected Countries.
| Country |
1990 |
1995 |
1998 |
|
| Lithuania |
26.1 |
45.6 |
42.0 |
|
| Estonia |
27.1 |
40.1 |
33.2 |
|
| Hungary |
39.9 |
32.9 |
32.1 |
|
| USA |
12.4 |
11.9 |
11.4 |
(1997) |
| Spain |
7.5 |
8.1 |
8.5 |
(1996) |
Source: World Health Organization.
The growing perception of suicide as a major public health
problem in Lithuania is important for this research because suicide is linked to
various diagnoses of mental illness, such as depression. Partly in reaction to
the high rate of suicide, a conference on depression was sponsored in 1995 in
the city of Kaunas. Furthermore, a national conference on suicide prevention
took place in Lithuania in 2000. From the Lithuanian government's point of view,
such a high suicide rate provides a mandate to seek cost-effective strategies
such as drug-based therapies, aimed at reducing suicide.
Changes in Health Care Structure
Since effective psychotherapy is potentially longer and
more expensive than drug therapy, the latter is favored by the government. As
one psychiatrist said,
...there was mandatory health insurance. This had the
effect of medicalizing the medical system. Medicine is medical—drug—
treatment, so there can be no psychotherapy.
Changes in health care reform favorably influenced
pharmaceutical companies' ability to sell their products. Prior to 1994, there
was no national health insurance in Lithuania. According to the first president
of the Lithuanian Psychiatric Association, since the passage of a 1995 law,
which promises all employed Lithuanians health coverage, there has been a
movement toward greater biological-medical treatment of mental health. As
Polubinskaya (2000) points out, there was a movement among psychiatrists in
Lithuania to make a conscious break with the past. The dean of the Vilnius
medical school explains,
I was the first head [of the Lithuanian Psychiatric
Association]. They wanted the young [doctors] to get involved. There's the
problem of stigma; during Soviet times, the mentally ill were locked up, now
they are deinstitutionalized. Society feels they should be locked away.
The "Sajudis" political movement, which sought independence
during Soviet rule and whose proponents ultimately came to power in the newly
democratic Lithuania, wanted progressive psychiatrists, such as the current dean
of the medical school, to steer Lithuania's practitioners away from Soviet-style
therapy. To illustrate his reformed practice, the dean placed a renewed emphasis
on psychotherapy and other forms of social and nonbiological therapy in
Lithuania.
The shift from psychotherapy to drugs is related to a shift
in government agencies, such as the Ministry of Health, toward private, rather
than governmental sources of funding. Also, embarking toward
deinstitutionalization of the mentally ill, the government is shifting to
medicines that deal with the most severe cases ("ambulatory" medicine), as
indicated by the reduction in the number of psychiatric hospital beds. Through
medication, physical restraints have been replaced by chemical ones. Drugs used
by Lithuanian doctors to treat affective mood disorders are now prescribed more
often, reflecting the increase in diagnosed disorders.
Influence of the Biomedical Model Under Soviet Rule
The biological model that dominated Soviet medicine viewed
psychiatric disorders as resulting from a breakdown in the organism itself
(Krethschmer, 1978). According to Marxist dialectical materialism, which was the
philosophical basis of Soviet ideology, in the Utopian workers' society (which
the Soviet Union claimed to be), there could be no social cause for mental
illness, hence the ideological search for biological causes of illness. A
biological breakdown in psychological functioning was treated with biological
means, as Miller (1985) clarifies:
Even before the 1917 revolution, psychiatric theory in
Russia, dominated by Kosakov and also by the work of Vladimir Bekhterev in
neurophysiology, was oriented around the notion that most mental disorders
were based on functional changes in cerebral activity or brain injuries of
various kinds (p.15).
The Soviets rejected Western models of psychology, such as
the Freudian, because they did not deny the influence of external factors on
mental health (Miller, 1985). As a result, Soviet psychiatry stressed the role
of biological and chemical forms of treatment (Wortis, 1950). This biomedical
approach has established societies that see the role of medication differently
than do Western societies.
Professional associations in Lithuania and other
post-Soviet countries are seeking new approaches to treatment. For example,
Polubinskaya (2000) affirms the intention of the Lithuanian Psychiatric
Association to "develop diagnostic and therapeutical [sic] approaches other than
biological psychiatry." Polubinskaya's work relates to my research by indicating
the legacy of the biomedical model in Lithuania and the LPA's attempt to move
away from biological psychiatry.
This Soviet predisposition to see mental illness as
something to be treated biologically, further enabled the drug companies to
market their products to the medical community. In elaboration of this view, a
Lithuanian psychiatrist told me:
The government seeks to augment the role of the
biological model in preventing suicide. It is funding suicide prevention in
the form of antidepressants.
The psychiatrist's reference to the "government" includes
agencies responsible for health care, but especially the Mi-nistry of Health.
Recent Changes in Psycho-pharmacology and Psychiatry
in Lithuania
It seems clear that the stage was set for drug companies to
enter Lithuania around the middle of the 1990s. According to a Baltic
representative for a Western pharmaceutical company, following the
disintegration of the Soviet Union, many corporations began conducting business
in the newly independent Baltic States to meet a need for insulin. In 1994, Eli
Lilly opened an office in Vilnius and began to market its products. The
expansion of drug companies into Lithuania had an impact on psychiatry as well.
The number of psychiatrists in Lithuania has been
relatively stable, perhaps due to informal benefits, while the numbers of other
specialists are in decline, as Table 4 indicates, following the strategy
employed by the Lithuanian health Program (http://www.sam.lt), a long-term goal
of the Lithuanian Ministry of Health is to increase the number of psychiatrists
from 230 to 250 by 2005. Table 4 indicates the changes in the number of various
types of health care professionals in Lithuania.
Table 4.
Number of Lithuanian Physicians by Specialties and Year.
| 1985 |
1990 |
1995 |
1996 |
1997 |
1998 |
Specialty
(Area and % Change)
1985-1998 |
| 418 |
552 |
543 |
531 |
530 |
503 |
Neurology (+16.9%) |
| 445 |
497 |
512 |
505 |
527 |
519 |
Psychiatry (+14.3%) |
| 1716 |
1960 |
1699 |
1666 |
1646 |
1583 |
Pediatrics (-8.4%) |
| 1693 |
1521 |
1371 |
1352 |
1340 |
1229 |
Surgery (-27.4%) |
| 364 |
287 |
255 |
253 |
243 |
229 |
Pulmonary disease (-59.0%) |
Source: Lithuanian Ministry of
Health.
As a whole, after reaching a high point in 1990—the year
prior to Lithuania's Independence—the number of physicians in Lithuania has
steadily decreased. This can be explained by a number of factors, including a
changing demographic structure in Lithuania. Table 5 shows the decreasing number
of 20 to 24 year-olds, roughly the age group that would be entering college or
medical school.
Table 5.
Lithuanians Aged 20-24 During Selected Years, in Thousands.
| Year |
1985 |
1990 |
1995 |
1999 |
| Number |
297 |
276.9 |
283.7 |
259.8 |
Source: Lithuanian Ministry of
Health.
Due to this demographic shift, fewer students will finish
medical school and go to work as doctors, or enter medical school at all. The
relevant conclusion of Table 4 is that, while the number of specialists in
various fields are decreasing, psychiatry is one of the few specialties that
seems to be maintaining its numbers. One explanation for this is the desire for
doctors to enter a field fostered by the government. Despite a decrease in 20 to
24 year-olds, there has been no decrease in the number of psychiatrists. Yet
another explanation is the role of well-paying foreign drug companies vying for
medical school graduates. As the medical school dean indicates, there are
competing interests for those that potentially may be entering psychiatry,
"Doctors that graduate here [from Vilnius Medical School] and work for drug
companies earn five times as much as [those] working at a hospital—it is a dream
for them."
Another interesting conclusion relates to the surprisingly
small number of physicians entering cardiovascular medicine. According to the
Ministry of Health, heart disease accounts for approximately one half of total
mortality. Given this high rate, one would imagine the number of physicians
entering the field to dramatically increase, not decrease.
The expected rise in Lithuanian psychiatric specialists
would lead one to predict a further rise in affective mood disorders in the near
future. With more psychiatrists entering the health care system, one would
predict that there will be an overall increase in diagnoses. In the coming
years, with predicted increases in the number of psychiatrists, a continued
increase in the diagnosis of mental illness would not be surprising.
CONCLUSION
In summary, my research reveals the connection between
economic factors and the increasing diagnosis of depression in Lithuania. The
primary reason for the increase in diagnoses of depression is the influence of
Western drug companies, which have managed to sell their products in Lithuania
for three reasons: the government's need to save money, the prior dominance of
the medical model, and the perception of suicide as a major public health
problem.
Three general conclusions can be drawn from this research.
First, the relationship between drug companies and the Ministry of Health is
called into question. In young democracies, such as those in the former Soviet
republics, business and social welfare must remain distinct. Second, increasing
medicalization allows more power to fall into the hands of the medical
professionals, who, as was indicated, are closely tied to market forces. As this
research indicates, mental illness is a label which is all too easily applied.
When individuals are led to believe that they are sick, their entire lives are
affected. A third implication of this research relates to the consequences of
medicating a population for the sake of profit. Anyone who has noted the side
effects listed for common psychoactive drugs sees that often the physiological
effects, such as sexual problems, tremor and in the case of Zoloft, feeling
unusually sleepy, may be just as serious as the symptoms the drug was taken to
relieve.
Lithuania is an ideal market for pharmaceutical companies.
Of course, there may be a positive aspect to the presence of drug companies in
Lithuania: Sick people are treated with quality medicine. Nonetheless,
medicalization can be abused, and patients who could be treated through talking
forms of psychotherapy may be overmedicated to their detriment.
My research contributes to the field of social psychiatry
by linking capitalist economic influences to the rates of mental health
diagnosis. Under capitalism, psychopharmaceutical companies operate for a
profit. In order for drug companies to realize a profit, they must make sure
that patients are diagnosed with mental illnesses treatable by psychotropic
drugs. Mental health, therefore, is an arbitrary condition closely tied to
economic factors: under capitalism, where profit is paramount, diseases, such as
anxiety disorders, are marketed to their fullest extent by drug companies and
psychiatrists.
My research indicates a connection between capitalism and
the increasing diagnosis of mental illness in Lithuania. We are forced to
consider the role of the economy in creating disorders and illnesses from thin
air. Medicine, as a profession, rose to prominence only in the later half of the
last century, yet today it holds a legitimacy that rivals hard science. We must
remain skeptical of the objectivity of medicine, since, as this research
indicates, those who practice medicine—the physicians themselves—are greatly
influenced by market forces.
REFERENCES
Chase-Dunn, C. 1982. "Socialist States in the World Economy." In Chase-Dunn
(ed.), Socialist States in the World Economy. Beverly Hills, Ca.: Sage.
-------- and Boswell, T., 1998. "Post-Communism and the Global Commonwealth."
The Humbolt Journal of Social Relations. 24:195-219.
Foucault, M. 1965. Madness and Civilization, (trans.) R. Howard. New York:
International University Press.
Freud, S. 1917/1957. Mourning and Melancholia. London: Hogarth Press.
Garfield, S. 1994. "Research on client variables in psychotherapy." In S.L.
Garfield and A.E. Bergin (eds), Handbook of Psychotherapy and Behavior Change.
(Fourth Edition, pp. 190-228). New York: John Wiley and Sons.
Gosden, R. 1997. "The Medicalization of Deviance." Social Alternatives.
16, 58-60.
Habermas, J. 1989. The Theory of Communicative Action. 2 vols. Oxford, Polity
Press.
Heilbroner, R. 1985. The Nature and Logic of Capitalism. New York:
Norton.
Karp, D. 1996. Speaking of Sadness: Depression, Disconnection, and the
Meaning of Illness. New York: Oxford University Press.
Kraeplin, E. 1913/1962.
One Hundred Years of Psychiatry. New York: Philosophical Library.
Kretschmer, W. 1978. "Psychiatry in the Soviet Union."
Ost-Europa. 28, 310-317.
Laing, R.D. 1967. The Politics of Experience, and The Bird of Paradise.
Harmondsworth, England: Penguin Books.
--------. 1969. The Self and Others. New York: Pantheon Books.
Lavretsky, H. 1998. "The Russian Concept of Schizophrenia: A Review of the
Literature." Schizophrenia Bulletin. 24, 537-557.
Marx, K. 1848/1967. The Communist Manifesto. Harmondsworth: Penguin.
--------. 1848/1967. Capital. New York: Modern Library.
Mechanic, D. 1968. Medical Society. A Selective View. New York: Free
Press.
Mirowsky, J. and Ross, C. 1989. "Psychiatric Diagnosis as Reified Measurement."
Journal of Health and Social Behavior. 30, 11-25.
Polanyi, K. 1944. The Great Transformation: The Political and Economic Origin
of our Time. London: Routledge and Kegan Paul.
Polubinskaya, S. 2000. "Reform in Psychiatry in Post-Soviet Countries." Acta
Psychiatr Scand Supplement. 399: 106-108.
Ragin, C. and Becker, H. 1992. What is a Case? Exploring the Foundations of
Social Inquiry. New York: Cambirdge University Press.
Sands, R. 1983. "The DSM-III and Psychiatric Nosology: A Critique from the
Labeling Perspective." California Sociologist. 6, 77-87.
Scull, A. 1979. Museums of Madness: The Social Organization of Insanity in
Nineteenth Century England. New York: St. Martin's
Press.
--------. 1992. "The Matter of Madness: Perspectives on the History of
Psychiatry." Journal of the History of the Behavioral Sciences. 28,
234-240.
--------. 1996. Masters of Bedlam: The Transformation of the
Mad-Doctoring Trade. Princeton, N.J.: Princeton University Press.
Statistical Yearbook of Lithuania: 1999. Vilnius, Lithuania:
Methodological Publishing Center.
Szasz, T. 1961. The Myth of Mental Illness: Foundations of a Theory of
Personal Conduct. New York: Harper and Row.
Turner, B. 1995. Medical Power and Social Knowledge. Thousand Oaks: Sage.
U'ren, R. 1997. "Psychiatry and Capitalism." The Journal of Mind and Behavior.
18, 1-12.
Wortis, J. 1950. Soviet Psychiatry. Baltimore: The Williams and Wilkins Company.
Zborowski, M. 1952. Life is With People. New York: Schocken Books